Download and print the PDF or read the accessible version:
Appendix 9 contains a template safety plan for adult victim survivors which can include safety planning for children through the non-offending parent/carer.
Appendix 10 contains a template safety plan that can be used directly with older children or young people.
4. Intermediate risk management
4.1 Overview
This guide supports professionals to undertake risk management that responds to the presentation and level of family violence risk (seriousness), as identified through intermediate risk assessment (Responsibility 3).
Professionals should refer to the Foundation Knowledge Guide and Responsibilities 1–3 before commencing intermediate risk management. You should reflect on the Structured Professional Judgement model and applying an intersectional lens in particular (Responsibility 3 and Foundation Knowledge Guide Section 9.5) to inform your risk management approaches.
Key capabilities
This guide supports professionals to undertake intermediate risk management and includes:
- Working with victim survivors (adults, children and young people) to develop an appropriate risk management response based on their unique experience of risk and assessed level of risk.
- The different elements of intermediate risk management.
- Discussing staying at home or leaving and talking to adult victim survivors about their options.
- Responding to serious and immediate risk.
- Documenting evidence of family violence.
- Developing risk management strategies where there are multiple victim survivors, including children.
- Developing safety plans for children and young people, working with a parent/ carer (usually the mother) who is not a perpetrator (who may also be a victim survivor), and/or working directly with the child or young person.
You should use this guide:
- After an intermediate risk assessment (Responsibility 3) has been completed and family violence risk has been assessed as present.
- To develop risk management strategies and a safety plan in the first instance or to review and update an existing plan if family violence risk has changed and/or escalated.
Guidance on other elements of risk management including information sharing, referral and secondary consultation with other services is provided in Responsibilities 5, 6, 9 and 10.
Remember
Guidance which refers to a perpetrator in this guide is relevant if an adolescent is using family violence for the purposes of risk assessment with a victim survivor about their experience and the impact of violence. It does not refer to risk assessment and management for adolescents, which should always consider their age, developmental stage and individual circumstances, and include therapeutic responses, as required.
Professionals and services can take a wide range of actions to manage risk. The actions you take depend on your role, your organisation and the resources available to you.
4.2 What is risk management?
Risk management is a coordinated set of strategies and actions aimed at enhancing the safety of the victim survivor (adult, child or young person) and reducing or removing the likelihood that the perpetrator will commit further violence. All risk management must involve safety planning. In addition to safety planning, other forms of risk management may also be required such as discussing options with victim survivors, connection to support and services, secondary consultation, and ongoing risk assessment.
4.2.1 Elements of intermediate risk management
Intermediate risk management activities for victim survivors may include responding to a range of risks and associated needs. Key intermediate risk management actions you can take include:
- Responding to immediate risk (Section 4.5)
- Safety planning (including for children or young people) (Sections 4.6 and 4.8)
- Talking to victim survivors about options and connection to relevant services (Section 4.11)
- Ongoing risk assessment and management (monitoring for change and/or escalation) (Section 4.14).
Intermediate risk management is focused on immediate risk management and safety planning, which is outlined in this chapter.
Some intermediate risk management activities require engaging with other services for assessment and management activities, including information sharing. Practice guidance on undertaking these collaborative risk management activities is covered in:
- Responsibility 5: Seek consultation for comprehensive risk assessment, risk management and referral
- Responsibility 6: Contribute to information sharing with other services
- Responsibility 9: Contribute to coordinated risk management
- Responsibility 10: Collaborate for ongoing risk assessment and risk management.
Collaborative risk management processes increase the visibility of the perpetrator, facilitate more tailored responses and risk management strategies, and can be more timely and responsive to changes in the level of risk. These coordinated responses make victim survivors safer. Service providers who use collaborative risk management can also consider and access a range of risk management activities for victim survivors which may not be possible for services who work independently.
It’s important to continually review your assessment of risk and update risk management and safety plans, as risk levels can change quickly and at any time. Depending on your role, you may contribute to risk management in a short- term support or intervention or have an ongoing role. An ongoing role includes supporting monitoring of risk and continued collaboration with specialist services to support the victim survivor, share information, and/or maintain visibility on the perpetrator.
Remember
All professionals must still comply with their existing legal obligations, such as mandatory reporting to Child Protection (for relevant occupations) and the reporting of possible sexual abuse of children under 16 to Victoria Police (applies to all adults).
This guidance on risk management is consistent with these obligations and provides additional information on how to manage family violence risk in the context of these obligations.
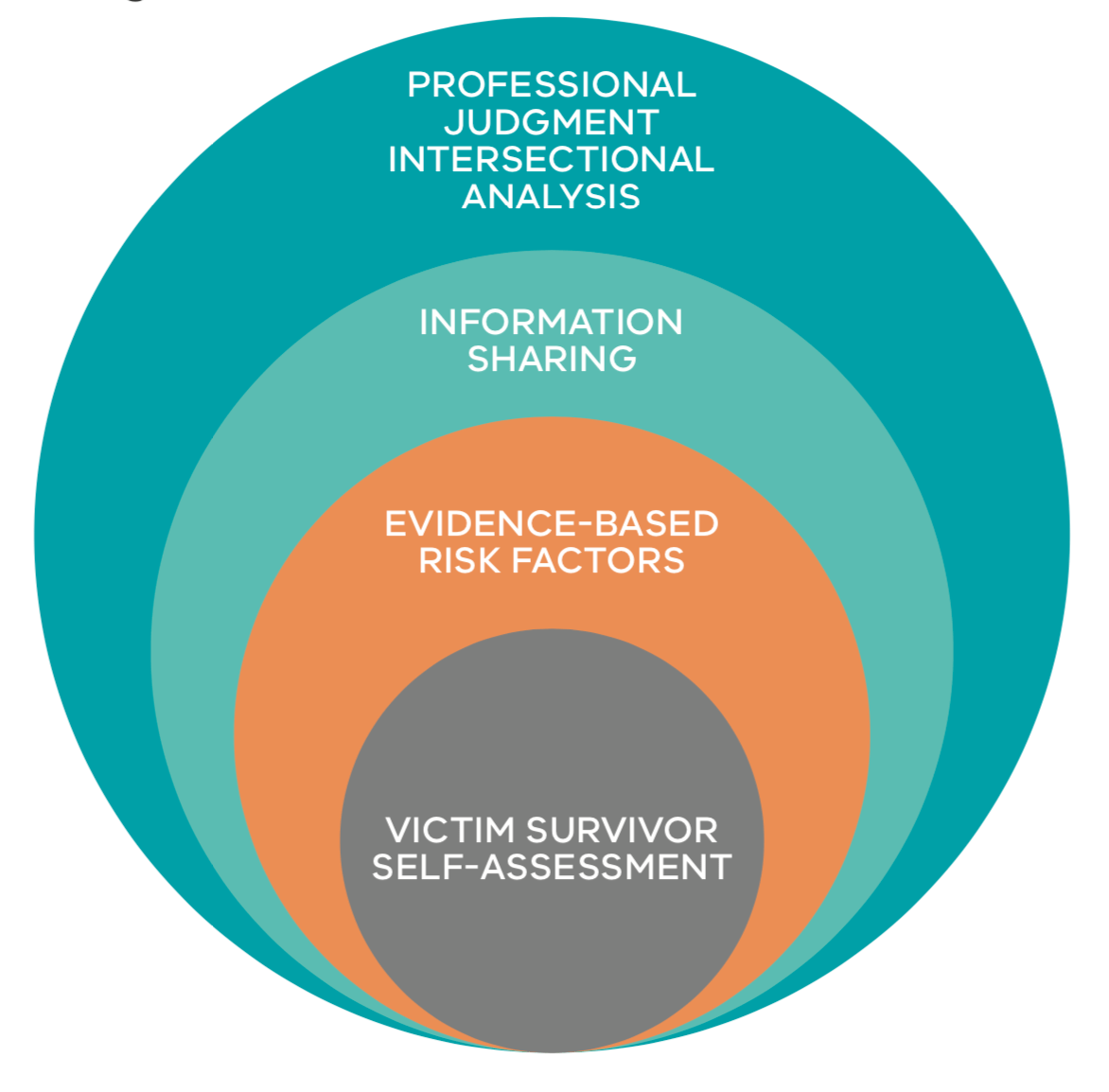
4.3 Structure professional judgement in risk management
Structured Professional Judgement supports you to respond through risk management actions to the level of risk you have determined through risk identification and assessment with the victim survivor and through information sharing.
Through the process of risk management at an intermediate level, you should:
- continue to keep the victim survivors wishes and needs central to your planned risk management actions
- respond to risk factors you have identified as present, particularly focussing on high risk factors and those identified as most impactful by the victim survivor
- continue to use information sharing with other professionals and services to ensure your risk management responses are relevant and support keeping perpetrators in view
Reflect through risk management on your intersectional analysis to respond to structural inequalities, barriers and discrimination a person may have informed you they have experienced throughout their life. These experiences will impact on:
- their experience of family violence from the perpetrator
- how they manage their risk and safety, and
- their access to risk management services and responses
Professionals should consider and make efforts to address any additional barriers for the person.
Your analysis of these elements and application of your professional experience, skills and knowledge support you to respond to the level and presentation of risk for each victim survivor.
Figure 1: Model of Structured Professional Judgement

{kind=link}
See guidance on secondary consultation, referral and information sharing in Responsibilities 5 and 6.
4.4 Starting the conversation about risk management
The victim survivor is an expert in their own life experiences and provides critical insight into the perpetrator’s attitudes, beliefs and behaviours.
You should recognise that the victim survivor has been taking actions to manage the risk posed by the perpetrator, including to any children who may also be victim survivors, and may have been doing so for a long period of time. The victim survivor will have likely tried many strategies to mitigate risk of violence and abuse, and its impacts. It is important to ask the victim survivor what has worked and what has not worked. We know that service involvement can be a protective factor. Therefore, ask what services or programs they have been involved with in the past.
You should start a conversation about risk management by telling the victim survivor that based on the outcome of the risk assessment you’ve undertaken, you need to work together to develop actions to support their safety.
You can begin by stating:
- “I’d like to talk to you about how we can assist to keep you (and your children, if applicable) safe.”
- “You have demonstrated strength and resilience in managing your own (and your family’s) safety — how have you done this in the past and how can we best support you with this?”
You can then ask the following questions:
- The behaviour of the perpetrator:
“Can you tell me about the impact his behaviour has had on you (and any children)?”
- The likelihood of the perpetrator repeating the behaviour:
“Can you tell me about what the pattern of behaviour has looked like in the past?”
- Service involvement:“
Can you tell me about any services that are currently supporting you or have been involved in the past?”
(These might have been legal, medical, educational, specialist family violence, housing/homelessness, AOD or mental health, disability, youth, Child FIRST or Child Protection?)
“What support did they provide to you?”
- Actions and strategies which the victim survivor has employed in the past:
“What has helped in the past that has kept you/you and your children safe?”
4.5 Responding to immediate risk
Actions to respond to immediate risk could involve:
Practice tip: Seek practice advice from a specialist family violence service.
- Contacting police (000) in crisis situations where an immediate response is required:
- You will be asked your name and where you are calling from
- Clearly explain who you are and your role, and why you are calling
- Give the full name of the victim survivor/s and their address and telephone number
- Give the full name of the perpetrator, (if known) their whereabouts and address
- Provide details about the situation, including about any crime that may have been committed, if known
- Report any risk posed to children or young people
- Provide any other information requested by the operator.
- A crisis situation may include both immediate risk from the perpetrator, as well as responding to immediate impacts from family violence, including medical response to serious/injury.
Remember
If loss of consciousness from strangulation or choking, or physical force to the head or neck is suspected or confirmed, you should seek an immediate health assessment for the victim survivor to ensure any injuries to the brain or body are responded to.
- Making a referral to a specialist family violence service, including for crisis or refuge response.
- Seeking secondary consultation from a specialist family violence service for comprehensive risk management planning or referring the victim survivor to a service for this support.
- If anyone discloses that the perpetrator has sexually assaulted a child, you have a statutory obligation to report to the police1:
- It is best practice to inform the adult victim survivor of your responsibility to report where possible. You can also reassure them that you can support them to ensure the safety of both the adult victim survivor and child from any increase in risk from the perpetrator that may occur as a result of the report
- Further practice advice about maintaining rapport and engagement can be found in Responsibility 1.
- Report the risk posed by the perpetrator to children or young people to Child FIRST/Child Protection and schools/ childcare centres (including sharing information regarding an intervention order if one is in place).
- Supporting an adult victim survivor to engage with legal services, and to make an application for:
- A family violence intervention order including for children and young people (if applicable).
- A personal safety intervention order, if appropriate, for community-based family violence or in family-like relationships, where the victim survivor does not want to apply for a family violence intervention order.
Remember
When making decisions on what course of action you should take, it is important to talk to the victim survivor about who you are contacting to seek assistance and who you are sharing information with.
You should seek the views of an adult or child victim survivor/s about sharing information about a child or young person’s risk wellbeing or needs, unless it is not appropriate, safe or reasonable to do so in the circumstances.
4.6 Safety planning with an adult victim survivor
Safety planning is thinking about practical actions a victim survivor (and/or services) can take to be safer when living with family violence.
The process looks at the current situation and assesses what steps and strategies can be put in place to mitigate risk. A safety plan must be current, relevant, adaptable and kept up-to-date in response to change in circumstances.
It is important that safety planning is discussed in a way that does not make the victim survivor feel that family violence risk or its impacts are their fault.
A safety plan may be developed by professionals who have undertaken an intermediate risk assessment, or in collaboration with, or by, a specialist family violence service (see Responsibilities 5 and 6). If a specialist family violence service is not involved, you must develop a safety plan with the victim survivor.
Where family violence risk has been identified, all victim survivors, including children and young people, benefit from having a safety plan. This supports them to know what to do if risk changes or escalates.
4.6.1 When to do a safety plan
Safety planning should be undertaken:
- Where any level of risk is present, noting that the safety plan will differ depending on the level of risk identified.
- In collaboration with the adult victim survivor, including in the development, implementation and monitoring of the plan. It may be appropriate to work with a young person to develop their own personal safety plan.
- With the adult victim survivor to develop separate safety plans for each child or young person (if not being done separately), and to reflect these plans in the adult victim survivor’s plan, if appropriate2.
All risk management must involve safety planning, and it’s key that the victim survivor participates in and understands this process. Safety planning must occur whenever family violence risk is identified and assessed and should be updated whenever there are changes or escalation in family violence.
Ensure safety plans reflect risks and management responses of each family member so that each family member’s plan supports safety requirements for each individual as well as the family unit. You also need to ask what constraints/circumstances may impact the victim survivor’s capacity to implement a safety plan.
The safety plan must be documented and should be regularly updated to reflect changes in circumstances and risk levels. Any referrals made, or secondary consultations undertaken as part of risk management should be incorporated and documented as part of safety planning. For more information, see Responsibility 5.
4.6.2 Developing a safety plan — key elements
A template safety plan is available in Appendix 9.
Each safety plan is unique to the needs of the victim survivor and should be informed by their views on what will and won’t work. It can be empowering for the victim survivor if you recognise and affirm the successful actions and strategies a victim survivor has already used in the safety plan you develop with them. Actions that are helpful in some situations might inadvertently increase their risk in other situations. You should be guided by the victim survivor on what strategies will work best in their situation.
Safety planning involves talking with the victim survivor (adult, child or young person, if appropriate) about their living and travel arrangements, community connections, financial resources and other circumstances and arrangements that support safety for themselves and their children. Each victim survivor’s circumstances are different and safety planning can cover some or all of the areas below.
A safety plan for adults should (as appropriate):
- List emergency contact numbers.
- List the contact numbers for a specialist family violence organisation, including if an Aboriginal organisation or other culturally appropriate service is being engaged.
- Identify a safe place for the victim survivor to go if they are in danger, and how to get there.
- Reflect protective factors, incorporated from what the victim survivor has discussed with you.
- Identify a friend, family member or neighbour who can assist in an emergency, and how to contact them.
- Identify a way for the victim survivor to get access to money in an emergency.
- List what to include in an ‘escape bag’ or identify a place to store valuables, so that the victim survivor can access them when needed. An escape bag at a minimum should include:
- phone/communication devices
- keys (house, car, office, etc.)
- money (cash and coins), bank cards (if the account is not shared with a perpetrator)
- medications/scripts and important documents (or copies)
- clothing for themselves and any children or person in their care
- Identify ways to safely use technology, including e-safety strategies, and the limitations of devices used, including children’s devices.
- Specifically address any barriers to the victim survivor implementing the safety plan (for example, access to funds, access to vehicles, leaving a pet behind, or having mobility or communication difficulties).
- Explore necessary ties to community, such as caring responsibilities, access to medical care, education (particularly for children and young people), access to cultural organisations or faith places, or requirements to contact justice services (e.g. parole officer).
- Consider support needs: disability support, medical care, translation, systems literacy (such as being primary person engaging with Medicare, banks and Centrelink), financial literacy or access (if usually provided by the perpetrator).
4.7 Mandatory reporting to child protection and referral to child first
Reflect on your reporting obligations that are an existing part of your professional role.
Remember
Use of the MARAM Framework andMARAM Practice Guides are in addition to existing legal obligations, including mandatory reporting to Child Protection and professionals with obligations to refer to Child FIRST.
Where it is safe, appropriate and reasonable, involve a parent who is not a perpetrator in the referral or reporting process. You can use your professional judgement to determine this — and consider how to assist them to continue engaging with your service and support them in this process. This will contribute to a person-centred approach (see Foundation Knowledge Guide Section 9.3) and partnering with victim survivors.
4.7.1 Reporting to Child Protection or child and family services
Always make a report to Child Protection if you have a significant concern that a child needs protection. Professionals should consult their organisation’s policies on making reports to Child Protection for guidance on circumstances and factors to consider.
Medical practitioners, nurses, midwives, teachers (including early childhood teachers) and school principals, and police are mandatory reporters under the Children, Youth and Families Act 2005 (CYFA) (section 182). Mandated reporters must make a report to Child Protection if they form a belief on reasonable grounds that a child is in need of protection from physical injury or sexual abuse, and that the child’s parents are unable or unwilling to protect the child from that abuse.
From March 2019, out-of-home care workers, early childhood workers, social workers, registered psychologists and youth justice workers become mandated reporters. From early 2020, school counsellors will also be included.
If the child is Aboriginal or Torres Strait Islander, ensure this information is contained in the report from your service to Child Protection. This ensures that the Aboriginal Child Specialist Advice and Support Service (ACSASS) is notified and that cultural supports are put in place.
Make a referral to child and family services, such as Child FIRST, if you have significant concerns for the wellbeing of a child or an unborn child after their birth. Consider making a referral if wellbeing or needs issues are identified AND the child’s safety is not compromised (which would require a report to Child Protection).
4.8 Safety planning for a child or young person
Language in this section of ‘mother/carer’ refers to a parent/carer who is not using violence (not a perpetrator).
A template safety plan that can be used with an older child or young person is available in Appendix 10.
Refer to guidance on working with children and young people in Responsibility 3 for determining if it is safe, appropriate and reasonable to develop a safety plan:
-
Directly with a child or young person (using the plan in Appendix 10).
-
Through a parent/carer (usually the mother) in the adult safety plan template (Appendix 9).
You should consider safety planning needs for children and young people separately to an adult victim survivor. This will assist in identifying different experiences, risks and needs from adults and other children/ affected people in the family.
Each child’s experience of risk and safety/ needs is inextricably linked to that of the adult victim survivor/carer and other children in the family. Consequently, each child or young person’s plan must also take into account and work consistently with the safety plan of the adult victim survivor and other children or family members (as applicable).
There are two aspects to safety planning for a child or young person.
Where you are working with a mother/carer who may also be a victim survivor:
-
You need to work with them to develop a safety plan for each child in the family/ household affected by family violence. This can be recorded in the mother/ carer’s safety plan.
-
The primary focus of this plan for children will be about the child or young person’s immediate safety and removing them from harm.
Where you are working directly with a child or young person:
-
If appropriate, safe and reasonable (see Responsibility 3) you can fill out the child safety plan template with the child or young person. This will enable them to be actively involved and understand how they can also be active to support their own safety.
-
Older children and young people, like adult victim survivors, often take steps to manage their experience of risk which should be acknowledged and considered in how this can be included in the plan. The child’s safety plan will also focus on how they will act in response to and in addition to the mother/carer’s actions.
-
When talking with children and young people about their safety plan you should continue to focus on their experience of violence, reflect on how they have acted in the past to keep themselves safe and that it is not their fault.
-
As part of the safety plan for the child, as well as any adult victim survivor, you should discuss parenting arrangements and the relationship between a child and parent who is a perpetrator. This may apply whether the child’s mother/carer is in a relationship, has separated or the relationship has ended.
-
Each relationship scenario will alter the parenting arrangements that are in place for the child/ren in the family. If the relationship dynamics change at any point, this needs to be reflected with an update to the safety plan.
Record the key agreed details of each family member’s safety plan together to ensure they are consistent.
This can be included in the overall risk management plan.
It is important to note that the safety plan approach will need to be adjusted according to the age and developmental stage of the child or young person, as well as whether it is appropriate, safe and reasonable to develop a safety plan with them, or if planning should occur with a mother/carer present.
Table 4: Considerations for age and developmental levels in safety planning
|
Age |
Considerations3 |
|
|---|---|---|
|
Infants and younger children (0–5 years) |
May have their safety plan contained within the adult victim survivor/carer’s plan. |
When safety planning with young children (3–5 years) you should have the mother present. Affirming to the child that everyone wants them to be safe and they are not to blame are important messages for them to hear and for the mother/carer to deliver. Practice Tip: There may be times when a safety plan for a child under the age of 3 is needed. Children at this developmental stage should have their mother/carer with them for this discussion. Because the child at this developmental stage is often too young to openly discuss the safety plan, incorporate the child’s safety plan into that of their mother/carer. |
|
Older children and young people (6–18 years) |
The child or young person’s age and developmental stage will influence the level of involvement they have. They should be included in the development of their own safety plan wherever possible, including to reflect their views and wishes. This ensures they understand the purpose of the plan and enables them to feel empowered — providing a direct response to their experience of violence. If you cannot seek the views or input of the child or young person in the development of their plan, e.g. if the child is not present, you can develop safety plans on their behalf by talking with the mother/ carer who is not using violence. It also may not be possible to create a safety plan for a child or young person in consultation with a parent who is not using violence (generally the mother). In this situation, it is important to still consider the impact of your planning on any mother/carer in their life (who is not using violence). |
6–11 years of age: You can use the template plan with older children and young people of this age. Work with the child to define and understand what family violence is. Let them know that everyone wants the child to be safe. If you are working with both a mother/carer and child or young person, safety planning with children at this developmental level can be more effectively done with the mother/carer present. 12–14 years of age: You can use the template plan with older children and young people of this age. Another option is to create a simple written agreement with the young person stating what they could do and where they could go if they feel unsafe. You should ask the young person how much involvement they need or desire from the mother/carer in developing the safety plan. You can suggest they share their safety plan with their mother/carer. 15–18 years of age: The template plan for either a child and young person or adult can be used, working directly with the young person. Young people often have a greater ability to keep themselves safe but may need help in identifying their own resources and developing a realistic plan for themselves. You should ask the young person how much involvement they need or desire from the mother/carer in developing the safety plan. Suggest they share their safety plan with their mother/carer. At this age, males especially may feel they can protect their mother by intervening in the violence. While respecting their feelings, encourage discussion and state that this may put them and their mother at more risk — let them know that it is not the child’s responsibility and the father’s behaviour requires system intervention. |
4.8.1 Talking to child victim survivors about their parent who is a perpetrator
If the perpetrator is a parent/carer to a child, this can create complex and confusing relationships and situations for the child. Sometimes children aren’t sure what impact changes between their parents/carers as a result of family violence will have on their relationship with the parent who is a perpetrator. You should consider the following:
-
When engaging a child to complete a risk assessment or safety plan it is important to understand the tactics a parent who is a perpetrator (usually a father) may use to coerce a child or young person into providing and gathering information
-
The child or young person understanding what information they can talk with the perpetrator parent about. Some information may seem harmless but is used to monitor the parent/carer or child who is a victim survivor, such as their daily activities, where they go, who they spend time with/contact with other family or friends, or other questions
-
You (and the mother/carer who is a victim survivor) recognising that a child or young person may have strong loyalty to a parent/carer who is a perpetrator. This may impact on whether the child or young person feels it is ok to share information with them (whether voluntarily, without meaning to or in response to questions from a perpetrator)
-
You should consider the experience of the child in these circumstances and how their experience of trauma and cumulative harm can change their understanding of what is ‘normal’ or ‘ok’ to talk about with the perpetrator. For example, when they ask the child for information to monitor the mother/carer or other family members.
Your approach to discussing this issue with a child or young person will depend on their age and developmental stage. Sometimes it may be appropriate, safe and reasonable to have a conversation directly with the child (guidance in Table 4 on age and developmentally appropriate actions can support your decision-making around this).
Inform the child or young person that the purpose of the conversation is safety for them or other family members. It is important to recognise the experience and impacts of violence on children and young people in this situation. In any situation, you should let the child know:
-
That they will not be in trouble for telling information to the perpetrator and emphasise that they should let their parent who is not a perpetrator, yourself or another safe person know if they have done so
-
They are not responsible for any behaviour or violence from a perpetrator which occurs if the child does share information with the perpetrator.
Practice tip: If you are not trained in working with children or young people, or feel you need assistance on risk management or safety planning, you may wish to seek advice through secondary consultation with a specialist children’s worker or specialist family violence service for their advice and support in these activities (see Responsibilities 5 and 6).
As part of a safety plan with the child or young person, it is best practice to:
-
Ask the child if the perpetrator asks them questions about the parent who is a victim survivor, or anyone else in the family
-
Suggest ways the child or young person can respond to questions from the perpetrator that are attempting to monitor or seek information about the child or a parent/carer who is a victim survivor, to further perpetuate violence
-
You can also role play options with the child on responding to questions from the perpetrator to help them feel more prepared.
It is likely that at some point in time a child or young person will disclose information to a parent who is a perpetrator. This disclosure may change the level of risk if the perpetrator uses that information to further perpetrate violence. In these circumstances the risk assessment should be reviewed and risk management and safety plans be updated.
Practice tip: You should develop risk management and safety plans with the presumption that at some point in time the child or young person will disclose risk- relevant information to the perpetrator.
Ensure that the child or young person, and the adult victim survivor are prepared in this situation. This includes the child or young person being ready to tell their parent who is a victim survivor when this has happened or to let yourself or another safe adult know so that the risk can be appropriately managed.
4.9 Safety planning where an adolescent is using family violence
Safety planning if an adolescent is using family violence differs to planning in response to an adult perpetrator. This is because risk management for adolescents using family violence should always consider their age, developmental stage and individual circumstances, and include therapeutic responses, as required. This is particularly important if the adolescent is both using and experiencing family violence.
Safety planning with the adult victim survivor (usually the mother) will need to include discussion on the therapeutic and other needs of the adolescent and how safety can be enhanced for the whole family whilst also addressing these needs.
The adolescent’s safety plan is generally shared with the adult victim survivor, so they can support the adolescent to implement their safety plan. Permission is needed from the adolescent before this occurs.
Any safety plan undertaken with an adolescent using family violence should occur and be consistent with safety planning for other family members, including adult victim survivors (usually mothers) or children (usually siblings) who are the target of violence.
Where adolescents use family violence a safety plan for that adolescent may include:
-
List the contact numbers for support organisations they may be already linked with, including if targeted community services are being engaged and that they can call if they identify their ‘early warning’ signs for abuse and violence.
-
Reflect protective factors, discussed and incorporated from what the adolescent has shared with you. E.g. Practice calming exercises every morning.
-
Identify a safe place for the adolescent to go if they feel they may progress to using violence, and how to get there.
-
Identify a friend, family member or neighbour who can assist and how to contact them.
Safety planning for an adolescent using violence may involve strategies for the victim survivor to respond to the adolescent’s use of violence. This does not mean the adult victim survivor is responsible for the use of violence by the adolescent but does acknowledge their contribution to family safety.
You can seek secondary consultation on how to support parenting practices with parent/carers of adolescents using violence, to ensure they are supported to respond to the adolescent’s behaviours, including if there are other siblings in the home. These may include:
-
How to improve conflict management, how to respond to threats and how to protect other children or young people or family members.
-
Strategies to de-escalate the adolescent’s abusive behaviour. For example, by not ‘buying into’ arguments.
If an adolescent using violence has a cognitive or intellectual disability, a risk management plan may include supporting the adult victim survivor to access a service that can support them to learn and implement behaviour modification strategies.
If the victim survivor is a parent of an adolescent using violence, particularly if the adolescent is young and/or has a disability, it is often a less feasible option for a victim survivor to leave. Additional options include:
-
Exploring the possibility of respite for the adolescent (if they have a disability) to facilitate a ‘cool off’ time and provide an opportunity for an exploration of interventions the victim survivor can use to prevent and minimise the use of violence.
-
Exploring the possibility of the adolescent going to a youth refuge to ‘cool off’. The police or a youth support service may be able to assist.
-
Exploring with the victim survivor the triggers, if any, which may lead to the use of family violence and how to avoid ‘triggering’ the adolescent or making changes to parenting and communication. This does not mean telling the victim survivor to rescind their parenting role, but it can begin to explore the patterns of communication and relating between parent and adolescent that may support the use of violence.
4.10 Discussion about leaving or staying safe at home
Making a decision or beginning to plan to leave a relationship with a perpetrator is a high-risk time period for an escalation of, and/or change in violence, including increased risk of being killed or seriously harmed.
It is important to recognise that a victim survivor does not have control over the abuse they are experiencing from the perpetrator.
Some victim survivors face significant barriers to leaving violent relationships and remain at home or in a relationship out of legitimate fears about what might happen to them and their children if they leave. It is important not to blame the victim survivor for this decision, and to explore the barriers or reasons with them. Some common, often interrelated reasons include:
-
Fear of escalation of violence.
-
Self-esteem (which may be significantly diminished from violence, trauma and abuse, shame at failure of relationship and guilt or self-blame about the abuse experienced).
-
Housing security, access to money/ financial security.
-
Keeping the family unit together (this may be internal and/or external pressure) — or have caring responsibilities for the person using violence (such as an adolescent).
-
Belief and hope that the perpetrator will change.
-
Isolation (family and support networks).
-
Lack of transport and means of communication.
-
Cultural and social expectations.
-
Concerns about what will happen to the perpetrator.
If a victim survivor has expressed a desire to stay in the relationship or family home, explore some of these reasons. If the reasons are based on barriers to leaving, you can ask whether they would like support to overcome these barriers.
If the person is not ready to leave a relationship and/or planning to leave may take time, you can explore options for them to remain more safely in the home. These include action in the safety plan (outlined above), and may also include:
-
Being ready to call police on ‘000’ and/or crisis specialist family violence services.
-
If the victim survivor feels the situation is escalating which might lead to violence, try moving to a space that is lower risk — avoid bathrooms, garages, kitchens, or other locations where there are objects or weapons available, or spaces where violence has previously occurred.
-
Plan possible escape routes from every room in the house, practice escapes and have window and door keys readily available.
-
Talk to the children about what is happening and encourage them to call for help and not intervene if violence occurs. Emergency numbers may be programmed into the phone or an older child or young person’s phone. They should never use a phone to call for help in front of the perpetrator as this may endanger them further. Make sure they know their safety plan actions if violence occurs.
-
Create code words or phrases for trusted friends or children so they know when to call for help and/or leave danger areas.
-
Choose a place to go — and let the children know where this is if you are separated. Let trusted friends/family know the safe place.
If they have decided that leaving is the best option, advise them that you or a specialist family violence service can help make plans to leave for a safe place. You should discuss whether it is safe to tell the perpetrator that they are leaving. If it is not, discuss when might be a safe time to leave. For example, when the perpetrator is not at the family home, at work, or away, or when the victim survivor has to leave the family home for a reason perceived as ‘legitimate’ by the perpetrator, such as picking the children up from school, going to a medical appointment, or going to work.
4.11 Talking to adult victim survivors about their options
Assist the victim survivor to identify and consider their options for support in a collaborative manner. Risk management and safety planning should be person-centred and victim-led, supporting each plan’s feasibility, safety and implementation (see Foundation Knowledge Guide Section 9.3).
Often, improving broader wellbeing or responding to needs, such as responding to the impact of a perpetrator’s behaviours, can improve effectiveness of risk management and safety plans, and support stabilisation and recovery from violence. These elements are reflected in the protective factors outlined in Responsibility 3, and the safety planning template at Appendix 9.
If making referrals, explore barriers to utilising referrals. Barriers will be different for each victim survivor and may be based on:
-
Their personal goals or interests and those of their children (for example, housing security, connection to community, culture, identity, family and friends).
-
Their experience of services in the past or experiences of structural inequality or discrimination (for example, poor engagement or response from services).
Many victim survivors may not feel ready to accept a referral, but by talking about barriers and options, you will have let them know that there is assistance available. You may also be able to reduce or remove barriers by facilitating warm/active referral and information sharing to limit a victim survivor having to retell their story. This is further outlined in Responsibility 5 and 6.
You could discuss:
What actions they have taken in the past to keep themselves safe
- How they have demonstrated resilience or strength — “Are there things you have done in the past that you think helped keep you (and your children) safe?”
Barriers to service access
-
Ask if they have experienced discrimination or poor service response in the past. Do they identify as Aboriginal or belonging to a diverse community? (See Foundation Knowledge GuideSection 9.4 and 9.5). Consider if there are ways you can reassure the person about these barriers and experiences and respectfully acknowledge their identity and circumstances while doing do (see Responsibility 1)
-
Ask “Is there anything I can do to make the referral or connection to a service successful?” For example, for victim survivors who identify as gender non- conforming or transgender, you might want to ask if conveying this information with the next service could assist them in providing a safe environment. Other examples could include asking about communication and/or access supports for victim survivors with a disability or interpreters for culturally and linguistically diverse victim survivors
-
You can also seek secondary consultation rather than referral if working together with another service can support engagement and consistent support (see Responsibilities 5 and 6)
-
Victim survivors experiencing elder abuse or family violence from adolescents may hold concerns about what will happen to the person using violence (often their child). This can be a significant barrier to the victim survivor leaving or excluding the person from the home. These concerns should be explored with the victim survivor.
Current needs
- Reflect on the domains of protective factors to guide conversation around wellbeing and needs. These may be personal or practical around housing, transport, communication, etc
- What issues are most important to them right now, e.g. “What would help most to support you?”
Informal social support
- Explore social supports available, e.g. “Have you talked to anybody about the family violence? Who do you feel you can trust? Do you have a family member, friend or trusted person in the community that you could talk to?”
Formal supports
-
“Have you had any previous involvement from services?” “What was your experience?”
-
“Are you currently or would you like to receive support from a service provider who specialises in [...]” (targeted community support, family violence, counselling or financial support, housing, or other support service outlined further below)
-
If so, then they could be encouraged and supported to contact that service using a ‘warm referral’ process.
Legal needs
-
“Are you currently engaged with any legal services?” “Do you want advice about [...]?” (financial entitlements if they leave the relationship, parenting arrangements for children, child support, property division, separation or divorce etc)
-
“Are there any family violence intervention orders in place?” “What are the conditions of the order/s?” “If so, has the order been breached?”
-
Are there any ‘red flags’ around legal issues, for example:
-
“Has a crime been committed? Such as criminal damage?”
-
“Has anyone been charged with a crime?” (Note, some victim survivors may have criminal charges)
-
“Has the person made any threats to remove/limit access to children or leave the country?” (Consider checking who has access to children’s passports)
-
“Have any fines/infringements been incurred? If yes, has it been wrongly assigned to you?” Relief may be available even if the fine/infringement was made against a victim survivor if it is linked to their experience of family violence. Relief is also available to re- assign fines and infringements which were caused by the perpetrator’s behaviour. Consideration should be given where the perpetrator incurs fines that the victim survivor pays.
-
Practice tip: If you aren’t sure about how current legal processes work, you can contact a specialist family violence service or a legal service for assistance to understand options and how to manage risks.
Mental health needs
- “Some people experience impacts on their mental health from the violence. Is this something you’ve experienced? Would you like assistance with this?”
Parenting needs
- “It sounds like you have done a lot to keep yourself and your children safe. Even with these efforts, sometimes a perpetrator will undermine the relationship between a parent and children, or your parenting skills and abilities. Would you like assistance in strengthening your relationship with your children?”
Service supports for children and young people
- “Children and young people are often impacted by family violence in invisible or less well-recognised ways. Are there actions we can take together to support the child/young person?”
- Check in on children and young people’s health and wellbeing needs: “What things does the child/young person enjoy doing? Are they still able to do these activities? Do they get to see friends and family? Do they have another trusted adult? Do they have any immediate health needs?”
- “Do the children have any disability support needs I should be aware of when safety planning or connecting you to services?”
4.11.1 Information sharing
This is further outlined in Responsibility 6.
You should ask the victim survivor if they have any concerns about information being shared with individual professionals or services, or if there is information they are concerned will increase their risk if the source is known to the perpetrator. These concerns should be responded to and detailed in the safety and risk management plan. Recording this in each plan will ensure you and the victim survivor have a shared understanding of how their information is shared, or protected, as required in the circumstances.
4.11.2 Connection to relevant services
Guidance on making referrals and seeking secondary consultation is in Responsibility 5.
Guidance on information sharing is outlined in Responsibility 6, and the Family Violence or Child Information Sharing Guidelines.
-
Making connections for the victim survivor to relevant services involves:
-
Sharing information with other service providers engaged with the victim survivor (adult, child or young person) as authorised, such as under the Family Violence Information Sharing Scheme, Child Information Sharing Scheme or privacy law
-
Referral or coordinated risk assessment and management responses with specialist family violence services, such as for housing relocation for the victim survivor, or other available services, or the victim survivor’s personal support networks (as required)
-
Referring to support services to address co-occurring issues related to wellbeing and needs, such as drug and alcohol problems, mental health concerns, legal needs and housing/homelessness, as required.
When working directly with children and young people, keep in mind that most services require parental permission to engage with children and young people under the age of 18.
4.12 Responding to serious and immediate risk
If you or any other professional or service identifies a victim survivor at serious and imminent threat of harm from family violence, you or they should immediately:
-
Notify Victoria Police.
-
Contact the local specialist family violence services, based on the victim survivor’s current place of residence.
In cases of ‘serious risk and requires immediate protection’, the specialist service will respond to provide comprehensive risk management, often in coordination with Victoria Police and other justice responses.
If these responses are not successful, they may require a coordinated response by a referral to a Risk Assessment and Management Panel (RAMP). A RAMP is a formally convened meeting, held at a local level, of key agencies and organisations that increases the collective capacity and effectiveness of the service system to identify and respond to perpetrators that pose a serious risk, and to hold them responsible and accountable for their violence.
This contributes to the safety of adults and children at serious risk and allows a response with direct interventions to immediate threats from family violence.
4.13 Documenting evidence of family violence
Documenting evidence of family violence is an important way to support applications for intervention orders and breaches or other justice or civil processes. You should only suggest this if the victim survivor can do so in a safe way.
Documenting could increase risk if discovered by a perpetrator. If the victim survivor is in the home with a perpetrator, you may explore keeping the documenting evidence in a safe place outside of the home.
If safe to do so, you can guide the victim survivor on documenting their experience of family violence. This might include:
-
Photographing injuries.
-
Medical evidence (including of sexual assault by specialist services).
-
Evidence of financial abuse.
-
Recording or writing down what was said or done, including details on time, location and specific details including any witnesses.
-
Noting breaches of orders, such as communication or exclusion orders.
-
Evidence of stalking, including through apps and technology, telephone or in-person (or from a third party on the perpetrator’s behalf).
-
Noting evidence of behaviours that led to harm of children or impact of that harm on children.
Records that you keep as part of your work practices, such as case notes and emails, can also be important sources of documentation that can support victim survivors. This is also important in keeping the perpetrator in view and ensuring their behaviour and impact is visible in case notes. For example:
Client presents as homeless; she has had to move three times in the past year due to ex-partner’s repeated attempts to locate her in breach of existing intervention order.
4.14 Ongoing risk assessment and management
Guidance on collaborative ongoing risk assessment and management is outlined in Responsibility 10.
Each risk assessment is a point-in-time analysis of the present risk, which is based on information known at the time from current and past behaviours of the perpetrator.
Risk management includes ongoing/ repeated risk assessment to identify if family violence risk has changed or escalated. Updates to risk management strategies and safety plans may be required where there are changes or escalation to the level and presentation of risk behaviours.
All professionals can support monitoring the safety of victim survivors through regular checking in, asking about changes in circumstances or experience of violence, observing changes in behaviour, or considering a review of assessment information that has been received from other sources/services that (may) affect risk.
If your service is child-focused, make sure to check in regularly with the child and any staff who have regular contact with them, and pay attention to any changes in behaviour that may indicate a change in risk. Refer to Responsibility 2, Appendix 1 and Section 10.3 of the Foundation Knowledge Guide for more information about the impacts of family violence on children.
If you or other professionals or services have contact with the perpetrator, you can seek information to monitor the actions and behaviour of the perpetrator to inform your understanding on the level of risk. You can also ask the victim survivor through your ongoing communication and service engagement about any changes or escalation in violence and support them to report breaches of any intervention orders or parenting orders to police.
Support can also be provided through contact and sharing information with the police and agencies and organisations involved in supporting the victim survivor.
4.14.1 Monitor safety, and the completion of actions against plans
It is important that organisations share relevant information about the perpetrator’s actions, behaviour and circumstances and the experience and circumstances of a victim survivor (including children). This information will be used to update risk management and safety plans, and to further share this information with other relevant services, such as specialist family violence services. This is especially important when the level of risk has changed or escalated, such as change in frequency or severity of violence.
Each professional or service which has an action assigned to them should make the best efforts to complete that action and let a coordinating service know when they have done so.
4.15 What's next?
You may seek advice and information from specialist family violence services to develop risk management and safety plans with victim survivors. After hours, professionals may contact 24-hours specialist family violence services for information and advice. To identify local family violence services you can refer to The Lookout(opens in a new window) website, or contact 1800RESPECT (1800 737 732).
In some circumstances, it is appropriate to seek secondary consultation or referral to a specialist family violence service for comprehensive risk management. Secondary consultation or referral:
- Must occur if the assessed level of risk is ‘serious risk’ or ‘requires immediate protection.’
- May occur if the assessed level of risk is ‘elevated risk.'
You may still have a role if a comprehensive risk management and safety plan is developed by a specialist service. This may include implementing actions, monitoring of safety and information sharing.
Guidance on:
- Making referrals and seeking secondary consultation is outlined in Responsibility 5.
- Information sharing is outlined in Responsibility 6.
- Collaborative ongoing risk assessment and management is outlined in Responsibility 10.
4.15.1 Document in your organisation’s record management system
It is important that you document the following information in your service or organisation’s record management system:
- All risk management and safety plans you develop for each adult and child victim survivor.
- Case notes and any other relevant information about the victim survivor or perpetrator’s circumstances.
- Any reports to police or statutory authorities you have made responding to serious and immediate risk, or if you have a significant concern for a child and young person.
- Any referral and secondary consultation actions you undertake.
- Any information you share with other services or professionals.
- Any risk management actions assigned to you or other professionals.
1. See State of Victoria, 2018, Children, youth and families, Criminal offences to improve responses to sex abuse, available online.
2. In some situations, entirely separate plans for children and young people may be required.
3. Table information adapted from Ministry of Justice Canada, 2013, Safety Planning with Children and Youth: A Toolkit for Working with Children and Youth Exposed to Domestic Violence.
Updated